Free North Carolina 90 Form
Free North Carolina 90 Form
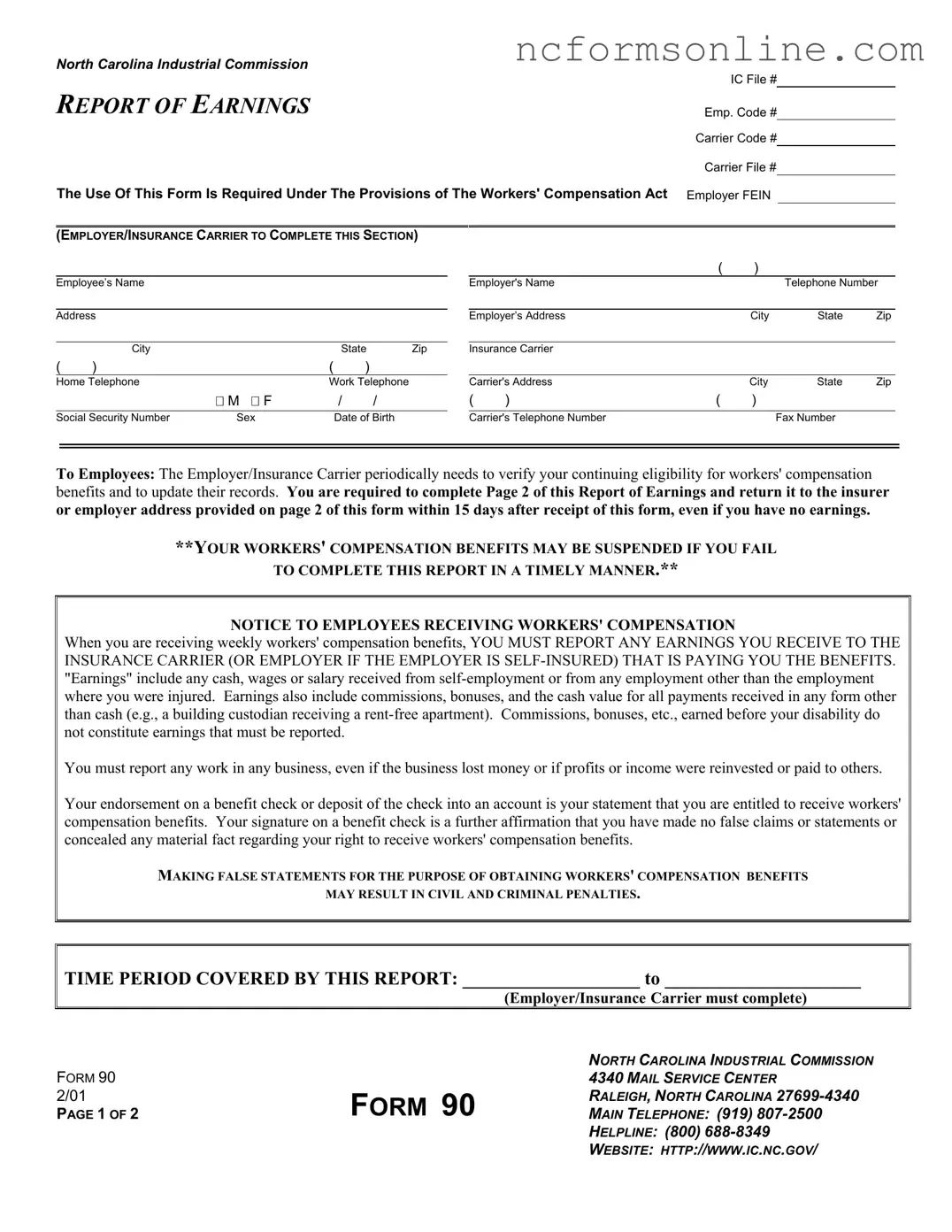
The North Carolina 90 form, also known as the Report of Earnings, plays a crucial role in the workers' compensation process for employees in the state. This form is designed to help both employers and insurance carriers verify an employee's ongoing eligibility for benefits while ensuring compliance with the state's Workers' Compensation Act. Employees are required to provide personal information, including their name, address, and Social Security number, along with details about any earnings they may have received during a specified time period. It's important to note that "earnings" encompass not only wages from traditional employment but also income from self-employment, commissions, and even non-cash benefits. By completing this form accurately and promptly, employees can avoid potential penalties, such as the suspension of their benefits. The form also emphasizes the necessity of reporting any earnings, even if they are minimal or from unsuccessful ventures, to maintain transparency and protect against civil and criminal liabilities. Understanding the requirements of the North Carolina 90 form is essential for both employees and employers to navigate the complexities of workers' compensation effectively.
NORTH CAROLINA INDUSTRIAL COMMISSION
IC File #
REPORT OF EARNINGS
Emp. Code #
Carrier Code #
Carrier File #
The Use Of This Form Is Required Under The Provisions of The Workers' Compensation Act Employer FEIN
(EMPLOYER/INSURANCE CARRIER TO COMPLETE THIS SECTION)
Employee’s Name
Address
|
City |
|
|
State |
Zip |
( |
) |
|
( |
) |
|
Home Telephone |
|
Work Telephone |
|||
|
|
M F |
|
/ |
/ |
|
|
|
|
||
Social Security Number |
Sex |
|
Date of Birth |
||
|
|
( |
) |
|
|
Employer's Name |
|
|
Telephone Number |
||
|
|
|
|
|
|
Employer’s Address |
|
City |
State |
Zip |
|
|
|
|
|
|
|
Insurance Carrier |
|
|
|
|
|
|
|
|
|
|
|
Carrier's Address |
|
City |
State |
Zip |
|
( |
) |
( |
) |
|
|
|
|
|
|
|
|
Carrier's Telephone Number |
|
|
Fax Number |
|
|
To Employees: The Employer/Insurance Carrier periodically needs to verify your continuing eligibility for workers' compensation benefits and to update their records. You are required to complete Page 2 of this Report of Earnings and return it to the insurer or employer address provided on page 2 of this form within 15 days after receipt of this form, even if you have no earnings.
**YOUR WORKERS' COMPENSATION BENEFITS MAY BE SUSPENDED IF YOU FAIL
TO COMPLETE THIS REPORT IN A TIMELY MANNER.**
NOTICE TO EMPLOYEES RECEIVING WORKERS' COMPENSATION
When you are receiving weekly workers' compensation benefits, YOU MUST REPORT ANY EARNINGS YOU RECEIVE TO THE INSURANCE CARRIER (OR EMPLOYER IF THE EMPLOYER IS
You must report any work in any business, even if the business lost money or if profits or income were reinvested or paid to others.
Your endorsement on a benefit check or deposit of the check into an account is your statement that you are entitled to receive workers' compensation benefits. Your signature on a benefit check is a further affirmation that you have made no false claims or statements or concealed any material fact regarding your right to receive workers' compensation benefits.
MAKING FALSE STATEMENTS FOR THE PURPOSE OF OBTAINING WORKERS' COMPENSATION BENEFITS
MAY RESULT IN CIVIL AND CRIMINAL PENALTIES.
TIME PERIOD COVERED BY THIS REPORT: ___________________ to _____________________
(Employer/Insurance Carrier must complete)
FORM 90 2/01
PAGE 1 OF 2
FORM 90
NORTH CAROLINA INDUSTRIAL COMMISSION
4340 MAIL SERVICE CENTER
RALEIGH, NORTH CAROLINA
MAIN TELEPHONE: (919)
HELPLINE: (800)
WEBSITE: HTTP://WWW.IC.NC.GOV/
EMPLOYEE: COMPLETE SECTION BELOW
(1) Did you receive earnings from work during the time period
indicated on Page 1? |
YES |
NO |
(2) Did you work for a business or any person during that time
period? |
YES |
NO |
(3)If you answered NO to both questions 1 and 2, sign and return the form to the insurance carrier or to the individual identified by the insurance carrier or employer listed below.
(4)If you answer YES to either question, complete item 5 below, sign and return the form to the insurance carrier or to the individual identified by the insurance carrier or employer listed below. For the purposes of this statement, “Gross Earnings” include all
(5)1st Employer or Business Name (include
Location:
Dates worked:
Gross Earnings:
Next Employer or Business Name (include
Location:
Dates worked:
Gross Earnings:
Attach additional page(s) if necessary.
Employee Signature: |
|
Date: |
|
. |
(Required)
NOTICE TO EMPLOYEE:
1.Failure to report earnings as defined herein may subject you to criminal prosecution and civil liability including the suspension or forfeiture of your benefits. This form must be signed and returned to the insurance carrier listed below even if you have no earnings.
2.If the Commission suspends benefits for failure to complete and return a Form 90 Report of Earnings, the
3.If benefits are not immediately reinstated, the employee should submit a written request for an Order from the Executive Secretary instructing the employer or insurance carrier to reinstate benefits. An application for reinstatement of benefits should be addressed to North Carolina Industrial Commission, Office of the Executive Secretary, 4333 Mail Service Center, Raleigh, NC
Insurance carrier or Employer must list the name and address below of the person to whom this form must be returned and mail this form to the employee by certified mail return receipt requested, and include a
Name: |
|
|
|
. |
||
Address: |
|
|
|
. |
||
|
|
City |
State |
Zip |
||
|
|
|
|
|
|
|
NOTICE TO INSURER OR EMPLOYER:
Any person who willfully makes a false statement or representation of a material fact for the purpose of denying or assisting another in denying any benefit or payment under the Workers’ Compensation Act shall be guilty of a Class 1 misdemeanor if the amount at issue is less than $1000. Violation is a Class H felony if the amount at issue exceeds $1000. Any person who threatens an employee with criminal prosecution under the provisions of the Act for the purpose of coercing or attempting to coerce an employee into agreeing to compensation under the Act shall be guilty of a Class H felony.
FORM 90 2/01
PAGE 2 OF 2
FORM 90
NORTH CAROLINA INDUSTRIAL COMMISSION
4340 MAIL SERVICE CENTER
RALEIGH, NORTH CAROLINA
MAIN TELEPHONE: (919)
HELPLINE: (800)
WEBSITE: HTTP://WWW.IC.NC.GOV/
| Fact Name | Details |
|---|---|
| Purpose | The North Carolina 90 form is used to report earnings for individuals receiving workers' compensation benefits. |
| Reporting Requirement | Employees must complete and return the form within 15 days, even if they have no earnings. |
| Legal Basis | This form is required under the North Carolina Workers' Compensation Act. |
| Consequences of Non-Compliance | Failure to report earnings can lead to suspension of benefits and potential civil or criminal penalties. |
Notice of Right to Have Exemptions Designated - Debtors can designate a portion of an unused homestead exemption towards other property types.
D422 - This form is required if you need to evaluate whether you owe a penalty for not paying enough estimated tax throughout the year.
The importance of having a legal document like the Florida Medical Power of Attorney cannot be overstated, as it ensures your healthcare decisions are made according to your wishes when you are unable to communicate them. By designating a trusted individual through this form, you can rest assured that your healthcare preferences will be honored. For those looking to establish such an agreement, you can find a suitable Medical Power of Attorney form to get started.
Workmans Comp Insurance Nc - Ensures a structured legal framework for addressing changes in family dynamics that might necessitate custody modifications.